 I've heard this question asked so many times by new patients, whether it be over the phone or during the initial examination. I always try to gently explain to people that we most often can begin treatment without needing radiographic imaging. Patients understand what I'm telling them and are willing to proceed with the recommended treatment I outline not because some belief that "I'm the doctor therefore I should always be trusted" but rather because I provide my patients with evidence based clinical decision making from credible research journals, state guidelines, position statements of well-known manual therapy associations, and my own clinical experience.
Recently I was shocked to learn that an article was published titled "X-Ray Imaging is Essential for Contemporary Chiropractic and Manual Therapy Spinal Rehabilitation: Radiography Increases Benefits and Reduces Risks" by Paul A. Oakley, Jerry M. Cuttler, Deed E. Harrison. In their article the authors “encourage routine use of radiography in manual spine therapy” and opine that “radiographic imaging is necessary to deliver acceptable patient care in the practice of contemporary manual therapy of the spine.” This belief that routine radiographic imaging (x-ray) is necessary to deliver acceptable patient care in the practice of contemporary manual therapy or that regular imaging is needed to improve the safety of manual therapy in general or spinal manipulative therapy are not true. No reputable clinical practice guideline or high-quality evidence suggest that radiological imaging is a routine requirement for effective treatment of back pain. In fact, the opposite is often the case; when imaging is performed, there is evidence that it does not improve patient outcomes but can result in undesirable and unintended effects. I agree that timely imaging in musculoskeletal health care is indicated by many clinical practice guidelines when clinical findings indicate suspected pathology (eg, fracture), when surgery is being considered, a patient is not responding to the standard treatment of care, or when a patient is routinely suffering the same chronic, recurring problem. This is not just my professional opinion but that of many other colleagues of mine including, The World Federation of Chiropractic Research Council. In Health, Dr Jared L Wilson, DC, MS References 1.National Institute for Health and Care Excellence: Clinical Guidelines (NICE). Low back pain and sciatica in over 16s: assessment and management | Guidance and guidelines. Natl Inst Heal Care Excell; 2016. 2.Qaseem, A, Wilt, TJ, McLean, RM, Forciea, MA; Clinical Guidelines Committee of the American College of Physicians. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166(7):514–530. doi:10.7326/M16-2367. 3.Stochkendahl, MJ, Kjaer, P, Hartvigsen, J. National Clinical Guidelines for non-surgical treatment of patients with recent onset low back pain or lumbar radiculopathy. Eur Spine J. 2018;27(1):60–75. doi:10.1007/s00586-017-5099-2. 4.Bussières, AE, Stewart, G, Al-Zoubi, F. Spinal manipulative therapy and other conservative treatments for low back pain: a guideline from the Canadian Chiropractic Guideline initiative. J Manipulative Physiol Ther. 2018;41(4):265–293. doi:10.1016/j.jmpt.2017.12.004. 5.Ash, LM, Modic, MT, Obuchowski, NA, Ross, JS, Brant-Zawadzki, MN, Grooff, PN. Effects of diagnostic information, per se, on patient outcomes in acute radiculopathy and low back pain. AJNR Am J Neuroradiol. 2008;29(6):1098–1103. doi:10.3174/ajnr.A0999. 6.Kendrick, D, Fielding, K, Bentley, E, Miller, P, Kerslake, R, Pringle, M. The role of radiography in primary care patients with low back pain of at least 6 weeks duration: a randomised (unblinded) controlled trial. Health Technol Assess. 2001;5(30):1–69. 7.Kerry, S, Hilton, S, Dundas, D, Rink, E, Oakeshott, P. Radiography for low back pain: a randomised controlled trial and observational study in primary care. Br J Gen Pract. 2002;52(479):469–474. 8.Djais, N, Kalim, H. The role of lumbar spine radiography in the outcomes of patients with simple acute low back pain. APLAR J Rheumatol. Wiley/Blackwell (10.1111). 2005;8:45–50. doi:10.1111/j.1479-8077.2005.00122.x.
1 Comment
 This New Blog post from Dr. Jared Wilson, DC, MS at Gaitway Chiropractic in Spokane, Washington discusses the mortality effects of being either unfit or fat. Dr. Jared Wilson blogs about chiropractic health and other relevant health news. He is an expert in musculoskeletal injuries and functional rehab. He holds a Chiropractic Doctorate degree and a Masters of Exercise and Sports Science degree.
Last year I posted this information to the Gaitway Chiropractic facebook page and I wanted to bring it up again in this health blog. In a recent meta-analysis (Barry et al 2014) researchers asked the question, " Which is a better predictor for death by all causes, cardiorespiratory fitness or fatness measured by one's BMI?" A meta-analysis is a study looking at a collection of other studies asking the same question in order to give a weighted average of the total effect. They determined that:
Bottom line conclusion from this article I think is we should be focused more on lifestyle modifications which include an increase in physical activity to be fit. This would improve a person's cardiorespiratory fitness and perhaps we should not be focusing too much on weight loss driven approaches to health. But let us not get carried away here. We know that being overweight and obese does increase your risk for disease. In another recent study (Vistisen et al 2014) of 6705 people, 35 to 55 years old, and an average follow up of 14 years, the researchers saw that 645 of those people developed diabetes. Of those 645 people, 94% were actually in the staying overweight group, 2% were in the progressively gaining weight group, and 4% were in the persistently obese group. The 6060 participants who remained free of diabetes were characterized by a mean BMI of just below 25 that rose only gradually over the follow-up period. At first glance it would appear that this second study possibly contradicts the first one and that being overweight and obese should be areas of concern. However, without knowing more information about the typical eating and exercise habits of the people in the second study it is difficult to correlate the two. Perhaps those who didn't get diabetes in the second study was due to the GRADUAL rise in BMI over the 14 years. It makes me wonder if these people were engaging in regular physical activity and if the people who got diabetes were mostly sedentary people. Hopefully you will find this information to be informative and most importantly motivating to live a healthy life by staying active and eating well. If you have any questions about how Dr. Wilson's expertise in Chiropractic, health, or sports medicine, please call Gaitway Chiropractic in north Spokane at (509) 466-1366, request an appointment online, or come by the clinic at 8611 N Division St, Ste A, Spokane, WA 99208. REFERENCES Barry, Vaughn W., Meghan Baruth, Michael W. Beets, J. Larry Durstine, Jihong Liu, and Steven N. Blair. "Fitness vs. Fatness on All-Cause Mortality: A Meta-Analysis." Progress in Cardiovascular Diseases 56.4 (2014): 382-90. Vistisen, Dorte, Daniel Witte, Adam Tabak, Christian Herder, Eric Brunner, Mika Kivimaki, and Kristine Faerch. "Patterns of Obesity Development before the Diagnosis of Type 2 Diabetes: The Whitehall II Cohort Study." PLoS Medicine 11.2 (2014): E1001602  This New Blog post from Dr. Jared Wilson, DC, MS at Gaitway Chiropractic in Spokane, Washington focuses on answering the question of how much protein should an athlete intake depending on the type of exercise, their state of training, and their gender. Dr. Jared Wilson blogs about chiropractic health and other relevant health news. He is an expert in musculoskeletal injuries and functional rehab. He holds a Chiropractic Doctorate degree and a Masters of Exercise and Sports Science degree.
Dating back as far as Ancient Greece and the Olympics, athletes have added protein to their diets to modify the effects of training on physique and performance. Conventional thought held by many athletes and coaches is that very high dietary protein intakes are needed to maximize protein metabolism within a muscle leading to faster repair and hypertrophy, the increase in cell size. But what does the current research suggest is the adequate amount of dietary protein intake for differing forms of exercise as well as the gender and performance level of the athlete? In this blog I will try to provide the answer in a comprehensive yet simple review on this hotly debated topic. Generally speaking, most athletes engaging in resistance exercise desire to increase their muscle mass, strength, and power. Whereas, endurance athletes are looking to augment longer duration output, such as increased maximal oxygen consumption, or reduce body fat. Now before I jump right into discussing adequate protein intakes for resistance exercise, I want to address endurance athletes first because even these athletes need to pay attention. Multiple studies have shown that endurance exercise increases the breakdown and utilization of protein for energy as you increase the intensity of the exercise and depending on the state of training of the athlete. A recent study by McKenzie et al evaluated protein usage in both male and female athletes during a 38-day high intensity endurance training program. They found that:
Other studies looking at athletes engaging in low to moderate intensity endurance exercise programs indicate that these athletes need the same amount of dietary protein intake or only slightly above that of a sedentary individual. So how much protein should an athlete consume given the intensity of their endurance workouts? Recreational endurance athletes who are exercising 4 to 5 times per week for 30 minutes below moderate to high intensities need about 0.80-1.0 grams of protein per kilogram of body weight per day. This is the same for sedentary men and women. Moderate intensity endurance athletes who are exercising 4 to 5 times per week for 45 to 60 minutes need about 1.2 grams of protein per kilogram of body weight per day. Elite high intensity endurance athletes (regular marathon runners and triathletes) need about 1.4-1.6 grams of protein per kilogram of body weight per day. And in general, dietary protein recommendations for female endurance athletes may be 10-20% lower than males. Surprisingly, these recommended values are much lower than the average protein intakes of most male and female endurance athletes. The typical male and female endurance athlete today consumes about 1.8 and 1.3 grams of protein per kilogram of body weight per day, respectively. So now that I’ve summarized the adequate protein intakes for endurance athletes let’s switch to protein requirements for resistance training athletes. First off, resistance exercise is different than endurance training in that a primary end goal is muscle hypertrophy or the increase in muscle size. Therefore it would only make sense that protein intake will need to be in excess that of basic sedentary requirements to provide the building blocks for muscle repair and growth, right? Well what does the research say? A study way back in 1988 by Tarnopolsky et al calculated how much protein intake it would take to match protein metabolism in 6 well-trained bodybuilders compared to 6 sedentary people. Surprisingly, they found that only 12% more protein intake was needed for the bodybuilders. Even more surprisingly, the bodybuilders were regularly consuming protein amounts of 2.7 grams of protein per kilogram of body weight per day which if you look back above you’ll find that this is 170% more the recommendations for sedentary people of 1.0 grams. (Also remember that recreational endurance athletes and sedentary individuals are at the same recommendation.) Now this study was looking at resistance athletes at steady state given the bodybuilders had at least 2 years of consistent training. The recommended protein intake for steady state resistance athletes is 1.0-1.2 grams of protein per kilogram of body weight per day. What about people in the early stages of resistance training? Do they need more or less protein intake? 4 years later Lemon et al answered this question by calculating the estimated protein requirement during the early stages of resistance training. They had 12 young men participate in 2 months of resistance training and split them into two groups having them intake either 1.4 or 2.6 grams of protein per kilogram of body weight per day. The men exercised 6 days per week for 2 hours each day. The weights were set to 70-85% the maximum weight that they could only do 1 repetition of. They found that the estimated protein requirement during this early stage of resistance training was 1.6 grams of protein per kilogram of body weight per day. Would you be surprised if I told you that the average resistance athlete today is consuming far more their needed protein requirements regardless of their stage of training in resistance exercise? Probably not since I’ve already told you this is true for two other situations above. The average resistance athlete today consumes 2.0 grams of protein per kilogram of body weight per day. This is 25% more than the amount needed for early resistance training athletes (1.6 grams) and about 80% more for steady stage resistance training athletes (1.1 grams). At this point I might be hearing a pour of outrage from some athletes believing they still need more protein to meet the demands of their resistance training, usually from the intense football or rugby player. So let’s look at the protein requirements for football and rugby athletes involved in weight-training and high-intensity sprinting and power activities as evaluated by the research of Tarnopolsky et al in 1992. They found that the protein requirement for this group at the highest was only 1.7 grams of protein per kilogram of body weight per day. This is only slightly higher than those athletes who are early on in their resistance training. So to recap, see below the listed protein requirements for the various athlete type measured in grams of protein per kilogram of body weight per day.
I know this is a lot of information but I hope you found this blog to be informative. Perhaps you will save some money on protein supplements or foods by knowing these recommendations. If you have any questions about how Dr. Wilson’s expertise in sports medicine could help you or have other Chiropractic questions, please call Gaitway Chiropractic in north Spokane at (509) 466-1366, request an appointment online, or come by the clinic at 8611 N Division St, Ste A, Spokane, WA 99208. REFERENCES Lemon PW, Tarnopolsky MA, MacDougall JD, Atkinson SA. Protein requirements and muscle mass/strength changes during intensive training in novice bodybuilders. J Appl Physiol 1992;73:767-75. McKenzie S, Phillips SM, Carter Sl, Lowther S, Gibala MJ, Tarnopolsky MA. Endurance exercise training attenuates leucine oxidation and BCOAD activation during exercise in humans. Am J Physiol endocrinol Metab 2000; 278:E580-7. Tarnopolsky MA, MacDougall JD, Atkinson SA. Influence of protein intake and training status on nitrogen balance and lean body mass. J Appl Physiol 1988;64:187-93. Tarnopolsky MA, Atkinson SA, MacDougall JD, Chesley A, Phillips S, Schwarcz HP. Evaluation of protein requirements for trained strength athletes. J Apply Physiol 1992;73:1986-95. 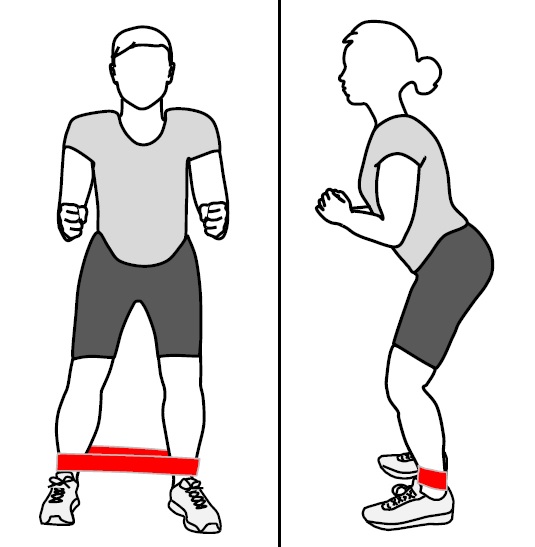 This New Blog post from Dr. Jared Wilson, DC, MS at Gaitway Chiropractic in Spokane, Washington looks to the research to answer if the posture or position taken when performing the resisted side-stepping exercise matters when trying to maximize gluteus medius activity and minimize tensor fascia lata (TFL) activity. Dr. Jared Wilson blogs about chiropractic health and other relevant health news. He is an expert in musculoskeletal injuries and functional rehab. He holds a Chiropractic Doctorate degree and a Masters of Exercise and Sports Science degree.
Hip abductor weakness is a common problem with people suffering from a variety of hip conditions such as femoroacetabular impingement, iliotibial band syndrome, and patellofemoral pain. It can even contribute to chronic ankle sprains. Weakness of the gluteus medius muscle will usually cause excess compensation from the TFL. Allowing the TFL to be recruited continually can lead to gluteus medius atrophy. Corrective exercises can increase gluteus medius strength and improve muscle firing patterns. Usually exercises involving a variation of resisted hip abduction are given. However, it is important for clinicians prescribing these exercises to be aware of excessive firing from the TFL when their patient is performing them. A recent study by Selkowitz et al (2013) looked at gluteus medius and TFL activation during 11 different exercises. The researchers used fine-wire electromyography (EMG) to determine the maximum voluntary isometric contraction (MVIC) of both the gluteus medius and TFL with each exercise. Their report showcased 5 exercises that activated the gluteus maximus and medius muscles without getting as much unwanted TFL activation. Those exercises included the clam exercise, single-leg bridge, hip extension (quadruped) with knee straight and knee bent, and the resisted side-stepping exercise. Specifically regarding the resisted side-stepping exercise, they found significantly lower TFL activation (13.1% MVIC) compared to gluteus medius activation (32.2% MVIC). Bottom line is resisted side-stepping should be included in any corrective exercise program designed to strengthen the hip abductors. But does the position or posture you take when performing the resisted side-stepping exercise matter? A study by Berry et al (2015) addressed this question. They had all 24 participants perform the exercise with an elastic resistance band around their ankles in both standing and squatting postures. Like the Selkowitz et al study, these researchers also used fine-wire EMG to determine the MVIC of the gluteus medius and TFL. Interestingly, they found that the EMG activity of the muscles being tested were actually higher in the stance leg rather than the moving one. They also saw that the EMG activity in the gluteus medius was significantly higher in the squat position than the upright position while activity in the TFL was lower in the squat position compared to the upright position. So to answer the question…yes! It does matter what position or posture you take when performing the resisted side-stepping exercise. Performing the resisted side-stepping exercise should be done in a squat position rather than an upright one. But how does this happen? Willcox and Burden (2013) gave a biomechanical explanation for the decreased TFL activity in the squat position. In the squat position the center of mass of the trunk is forward compared to the hip. This creates a hip flexion position and thus reduces the need to activate more muscles involved in hip flexion. Since the TFL acts also as a hip flexor in addition to being a hip abductor, the squat position would reduce the need to activate the TFL in order to stabilize the hip and pelvis. Increased TFL activation would be counterproductive. I hope you found this blog to be informative. If you have any questions about how chiropractic care could help you, please call Gaitway Chiropractic in north Spokane at (509) 466-1366, request an appointment online, or come by the clinic at 8611 N Division St, Ste A, Spokane, WA 99208. REFERENCES Selkowitz DM, Beneck GJ, Powers CM. Which exercises target the gluteal muscles while minimizing activation of the tensor fascia lata? electromyographic assessment using fine-wire electrodes. J Orthop Sports Phys Ther. 2013;43(2):54-64. Berry, Justin W., Theresa S. Lee, Hanna D. Foley, and Cara L. Lewis. "Resisted Side-Stepping: The Effect of Posture on Hip Abductor Muscle Activation." J Orthop Sports Phys Ther Journal of Orthopaedic & Sports Physical Therapy (2015): 1-30. Willcox EL, Burden AM. The influence of varying hip angle and pelvis position on 531 muscle recruitment patterns of the hip abductor muscles during the clam exercise. J 532 Orthop Sports Phys Ther. 2013;43(5):325-31. Image: Photographer unknown. (2015, August 6). Participant side-stepping to the right in the squat posture [digital image]. Retrieved from http://www.jospt.org/doi/pdfplus/10.2519/jospt.2015.5888  This New Blog post from Dr. Jared Wilson, DC, MS at Gaitway Chiropractic in Spokane, Washington addresses the importance of chiropractors and other medical professionals working together in a collaborative effort to improve patient-centered care. Dr. Jared Wilson blogs about chiropractic health and other relevant health news. He is an expert in musculoskeletal injuries and functional rehab. He holds a Chiropractic Doctorate degree and a Masters of Exercise and Sports Science degree.
Integrated care can have multiple definitions depending on who you talk to. Many people, including myself, would say that integrated care means that all providers (primary care doctor, orthopedist, physiatrist, chiropractor, physical therapist, neurologist, cardiologist, etc.) collaborate in a comprehensive, interprofessional, evidence-based, patient-centered effort to deliver effective and affordable care. This would give patients complete care. For this to work most efficiently though, there needs to be a system in place where providers are either able to, a) easily send office visit notes to a central location where the provider will actually see them; or, b) simply access the same electronic health record for that patient. This would allow all providers to see the big picture of the care being provided. You have this setup at a large organization such as Providence, Rockwood, Group Health. But chiropractors tend to be in an independent lot usually because the chiropractor is practicing in a private office setting and having all providers in the same space would improve communication. Plus hospitals and big organizations understand the value to them to keep loyal providers within their own system who regular refer patients within that system. Undoubtedly the greatest advantage of integrated care settings is patient care. However, I feel there is still a lack of effort put forth by many providers to strive for integration. The biggest reason, I believe, is time. Being part of a comprehensive care team requires more time and effort in communicating with other doctors. But I know that doctors who care about their patients will in fact take this time out of their busy schedules to meet their patients' needs. Coming out of chiropractic school I was blessed to work with an amazing chiropractor who modeled the very nature of patient-centered, integrative care. Any additional second he had away from treating patients was spent calling patients or their providers to ensure the best care was being given. This example really made an impression on me. Seeing patients benefit from this approach to their care is a reason I strive to do the same. Research shows that chiropractic care plays a critical role in pain management programs which reduce the long-term costs of health care. The Department of Veteran Affairs is a group that has seen the inclusion of chiropractic. The reason is the VA is following directives to find safe and effective alternatives to opiates and expensive surgical procedures. This has led to the gradual expansion of chiropractic services offered at the VA. This is great news! The easiest way I’ve found to integrate my care into a patient’s bigger care picture is simply asking new patients if they would mind me communicating their findings and treatment plan with their primary care physician. This is easily done by faxing initial office visit notes and follow up progress reports. I really think this is where the majority of chiropractors fit into the integrated patient care model. Not every chiropractor will have the opportunity to join with a major organization. The best part of integration is getting to see patients who never have received chiropractic care and wouldn’t have, for that matter, had it not been for their primary care doctor recommending it as a viable treatment option. If you ever hear a medical professional say, “Oh don’t go see a chiropractor,” I challenge you to ask them why? Writing this blog helps me stay motivated to continue reaching out to other providers, usually allopathic ones, in hopes to build healthy, interprofessional relationships. These types of relationships will help to break down any remaining ugly walls that may exist between the chiropractic and medical professions, reduce health care costs, and lead to patient centered care. Chiropractic care results speak for themselves. Anybody who doubts that can look at the piles of supporting anecdotal and clinical research. If you have any questions about how chiropractic care could help you, please call Gaitway Chiropractic in north Spokane at (509) 466-1366, request an appointment online, or come by the clinic at 8611 N Division St, Ste A, Spokane, WA 99208.  This New Blog post from Dr. Jared Wilson, DC, MS at Gaitway Chiropractic in Spokane, Washington addresses the importance of being evaluated by a doctor trained in whiplash biomechanics and traumatology after being involved in a motor vehicle collision. Dr. Jared Wilson blogs about chiropractic health and other relevant health news. He is an expert in musculoskeletal injuries and functional rehab. He holds a Chiropractic Doctorate degree and a Masters of Exercise and Sports Science degree. Over three million whiplash injuries occur each year in the U.S. as a result of motor vehicle collisions. Almost half of these injuries lead to chronic issues such as headaches, neck pain, back pain and shoulder pain, to name just a few. These problems can have significant impact on a person’s normal activities of daily living such as work proficiency, recreation, sleep, social interactions and more. Because of the unique presentation of these automobile collision injuries, it is important for the patient and the treating doctors to be educated about the many issues surrounding whiplash treatment and related medical-legal issues. Unfortunately many car accident victims suffer without knowing that there is much help available to them, often times at no cost to them. In order to address these issues and effectively treat persons injured in motor vehicle collisions, Dr. Jared Wilson has advanced education and experience in effective and efficient ways of treating these injuries. Dr. Wilson understands the wide range of physical injuries and clinical conditions that can occur as a result of these unfortunate events. At your first appointment at Gaitway Chiropractic, Dr. Wilson conducts a comprehensive physical examination. Dr. Wilson will even determine if your condition warrants the use of the latest imaging technologies such as dynamic X-Rays, CT, MRI, nerve conduction studies and others. He will make the proper referral for imaging when needed. Dr. Wilson is trained in how to provide patients with the most effective and comprehensive gentle treatment and rehabilitation strategies (including nutritional supplementation and diet instead of medication) to promote optimal healing. Dr. Wilson also recognizes when conservative treatment is limited, and he strives to put together the ultimate team of medical professionals that are focused on helping you recover from these motor vehicle injuries. To make an appointment, or ask any questions, please call Gaitway Chiropractic in north Spokane at (509) 466-1366, request an appointment online, or come by the clinic at 8611 N Division St, Ste A, Spokane, WA 99208.  Many people over the years have started using foam rollers in the gyms, health clinics, sporting events, and at home. You have probably seen your friends post on facebook, twitter, and pinterest the best ways to use a foam roller. The media has really helped increase the popularity of these self-myofascial release tools.
Over the past few years I've seen all kinds of posts on the internet about the right size, shape, and texture to use. The use of foam rollers has spread like wildflowers. You can even get one with flowers decorated on it, ha! But is this soft tissue therapy really helpful for the treatment of skeletal muscle issues like immobility, pain, loss of range of motion, and athletic performance? Let's turn to what the research indicates. A recent review of the literature was presented May 2015 at the American College of Sports Medicine 62nd Annual Meeting. Nine studies were evaluated. Six using foam rollers and three with handheld rollers. The findings?
Regardless of the exact mechanism of how myofascial release works to benefit skeletal muscle issues such as immobility, pain, loss of range of motion, and certain athletic performance measures, it is clear that it is beneficial. So call today, 509-466-1366, or request an appointment online and find out how to properly use a foam roller for you muscular complaints and what other ways we could help you. A new study by the department of social and behavioral health sciences at Harvard determined that more than half of all children and adolescents in the United States are not getting enough water. Could this be that we are drinking too much juices and soda throughout the day and thinking, "Well there's water in there so I must be okay."? There can be dramatic health risks to not getting enough water.
Severe dehydration can cause:
...But you may be surprised to know that even mild dehydration can result in
I always make sure that I get a full 20 fluid ounces in the morning before I eat anything and I force myself to get an additional 100 fluid ounces throughout the day. I keep my water bottle with my at all times. I like bottles that have measurement lines on the side so you can accurately determine how much you are getting. Did you know that drinking enough water can help you LOSE WEIGHT?! I tell people all the time who struggle with weight issues to drink HALF their weight in fluid ounces. This simple trick can help a lot in reaching your weight goal. “Prevalence of Inadequate Hydration among US Children and Disparities by Gender and Race/Ethnicity: National Health and Nutrition Examination Survey, 2009-2012,” Erica L. Kenney, Michael W. Long, Angie L. Cradock, Steven L. Gortmaker, American Journal of Public Health, online June 11, 2015, doi:10.2105/AJPH.2015.302572.  With the recent trend of cross fitness training in the early 2000's, and the growing interest in climbing sports, specifically rock climbing, elbow injuries along with other upper extremity injuries are becoming more prevalent.
Most often injuries to the elbow are to the biceps muscle. However a lesser but still common injury to the elbow is a strain of the brachialis muscle which is located close to the biceps and assists the biceps when bending the elbow. This injury is called Climber's Elbow. It is caused by a forceful flexion contraction of the muscle greater than it is able to tolerate or a forceful over extension of the elbow. Most often this injury, like most muscle injuries, are a result of a previous lesser strain to that muscle that likely never was caught or was not allowed to heal properly. The athlete then returned to full activity too early resulting in the injury. Diagnosis of Climber's Elbow begins with a clear understanding of the mechanism of injury. This comes from the patient's report of how the injury occurred. Using skilled palpation and specific muscle testing of the elbow in various positions, an expert in musculoskeletal injuries will be able to distinguish between the more common biceps strain and Climber's Elbow. Treatment of Climber's Elbow depends on the severity of the injury. A Grade 3 strain, a complete tear of the muscle away from its attachment point near the bone, is a surgical case. The less severe Grade 1 and 2 strains can be treated conservatively by a musculoskeletal injury expert. Below is a typical progression through the stages of healing for Climber's Elbow. Acute (Inflammatory) Stage (0-2 weeks)
Sub-acute (Repair) and Chronic (Remodeling) Stages (2-8 weeks)
It's important to note that the time frames listed above for the stages of healing for Climber's Elbow are just typical time frames. These would be the expected times only if the healing process occurs normally. Different body types, conditions, and compliance will effect this. Did you know that both the American Chronic Pain Association and the State of Oregon's low back pain management guidelines recommend SPINAL MANIPULATION as the only non-drug treatment for all three phases of low back pain (acute, subacute, chronic).
Chiropractic focuses on health, rather than disease. Prevention and wellness are at its foundation. Doctor Jared Wilson, DC, MS uses a "whole-person" style of chiropractic care. This includes spinal manipulation, soft tissue mobilization, functional corrective exercises, healthy lifestyle habit recommendations such as nutrition and exercise. This style of treatment can help healthy people stay healthy and offer those who are in pain the ability to regain health. The unique aspect of chiropractic is the manipulation of the spine and extremities using specific contacts and a controlled thrust with the hands, also known as an adjustment. An adjustment can help restore proper range of motion, nerve conduction and vascular flow as well as decrease pain and inflammation from injury and chronic pain syndromes. |
Dr. Jared Wilson, DC, MSDr. Jared Wilson blogs about chiropractic health and other relevant health news. He is an expert in musculoskeletal injuries and functional rehab. He holds a Chiropractic Doctorate degree and a Masters degree in Exercise and Sports Science. Archives
August 2023
Categories |
 RSS Feed
RSS Feed